


“USA250 : The Story of the World’s Greatest Economy” is a yearlong WSJ series examining America’s first 250 years. Read more about it from Editor in Chief Emma Tucker.
Diet is one of the three key components to a longer life (along with exercise and sleep), and it offers the highest and largest potential to change health and longevity.
That message, however, isn’t getting through.
Decades of information-based efforts to change people’s eating habits—via K-12 classroom education and prominent nutrition-information labels on packaged foods—has accomplished little. Too much unhealthy food and related chronic diseases rank among the biggest health challenges of the 21st century in the U.S. and many other countries.
To break this impasse, we are going to have to think outside the box. We need bolder action on several fronts, such as new types of health professionals that make nutrition their No. 1 priority and more effective dietary interventions, among other things.
When it comes to nutrition, science is converging on the following recommendations for longevity and health: a diet rich in vegetables, whole grains, nuts and plant-based unsaturated fats, moderate fruit and fish consumption, low red- and processed-meat consumption, and very low ultraprocessed foods and added sugars. While protein consumption gets a lot of attention, research suggests a low but sufficient daily intake of 0.37 gram per pound of body weight, or about 60 grams for a 150-pound person, of which at least 50% is plant-derived, is ideal.
None of that should be particularly surprising. And if more people embraced this type of eating we would have less disease and lower healthcare costs in the U.S. But they don’t.
With that in mind, here are some changes that we believe could move us closer to that goal:
A new kind of professional
The annual physical is obviously important for detecting disease but less so for preventing it. Doctors may provide generic nutrition advice during these one-hour visits, but they typically don’t have enough time to help overweight and obese patients, or even normal-weight patients, make dietary changes that can lead to a longer, healthier life. Registered dietitians, meanwhile, struggle to receive long-term reimbursement from health insurance at a level needed to make a difference.
To fix this, we are going to have to reimagine how we provide healthcare, putting more emphasis on lifestyle medicine. The ideal approach would include a multidisciplinary team of physicians, biologists, dietitians, psychologists, kinesiologists, etc., who, with the help of artificial intelligence, focus on reducing a patient’s biological age and with it age-related disease.
We also need a new category of healthcare professionals with graduate degrees obtained from accredited universities and institutes and whose training is centered on healthy longevity. Their focus would be on the role of nutrition—as well as exercise, sleep and other interventions—in maximizing a person’s “healthspan,” or the period of life spent in good health.
These professionals would evaluate therapies based on their predicted lifelong effects, not just short-term results.
Consider the weight-loss diets most often recommended by doctors today. Data show that many patients lose weight initially but gain it back over time, thus making their temporary weight loss futile and potentially detrimental. The same is true for GLP-1 drugs, which should be used only if lifestyle interventions fail.
Healthspan professionals would do things differently in that they would take the time to analyze (with the help of AI) which particular diets, drugs or procedures are likely to produce only temporary results and point physicians toward more-personalized therapies with a higher potential to optimize healthy aging.
Restricted eating
There are some novel science- and food-based interventions that have been proven safe and effective in achieving long-term reduction in aging and disease markers.
Specifically, we are referring to time-restricted-eating programs, in which people restrict their eating to certain hours of the day, and a fasting-mimicking diet, developed in our laboratory at the University of Southern California 15 years ago and tested in over 40 clinical trials. These programs aren’t draconian and don’t require people to be on lifelong restrictive diets, so sticking with them is easier.
A version of time-restricted eating that is particularly easy to adopt involves limiting food consumption to 11 to 12 hours a day and fasting for 12 to 13 hours a day. With these shorter daily fasting periods, it will take longer to lose fat and improve metabolism than versions of restricted eating that call for 16 hours of fasting. However, not only is this moderate version of TRE more feasible, it is safer because it doesn’t require skipping breakfast, which has consistently been associated with increased mortality. In addition to weight loss, the benefits of TRE include improved sleep and metabolic markers.
A fasting-mimicking diet, meanwhile, mimics a fast but instead of eliminating food entirely, you eat a low-calorie, low-protein, low-sugar but high-fat plant-based diet for a five-day period. Research suggests it may be effective in reducing biological age and disease risk factors when deployed for one cycle a month. Large studies are now under way to test the program’s effectiveness when done just one to four times a year, or five to 20 days in total.
The diet works by generating periodic resets, which involve metabolic reprogramming and, based on preclinical studies, also regenerative effects in multiple systems and organs. Multiple FMD cycles lead to fat loss with little or no lean-mass loss, promote A1C reduction and diabetes regression and have anti-inflammatory effects, including in patients with inflammatory bowel disease .
Treat food as medicine
That brings us to food. If we leave the responsibility of choosing a healthy diet solely in the hands of consumers, we are doomed to fail because the dietary choices people make are affected by a complex network of factors that extend beyond personal taste. Food packaging and placement, formulations, marketing and advertising, and sociocultural perceptions of norms and prestige created by the commercial market all play a role.
As such, it is vital that the government be willing to challenge some of the food industry’s focus on maximizing profits, especially if its products are contributing to diseases costing taxpayers trillions of dollars annually. We believe that advertising food clearly associated with obesity and disease to children should be banned, for example, and that labels on many ultraprocessed foods should warn of its dangers.
At the same time, governments could do more to help spur demand for healthy food, perhaps by using rebates or other financial incentives to make it more affordable, much like rebates were used to get more people to embrace electric cars and solar panels.
We also should consider treating food like medicine, with insurers and government payers reimbursing or heavily discounting healthy food and dietary programs that clearly lead to disease regression. If a GLP-1 is covered by insurance, but healthy food and a dietitian aren’t, patients will continue to choose drugs even if the effects are likely to be temporary and despite side effects.
We also believe there is room for more public and private investment in restaurants, grocery stores and companies that bring healthy food to the public. That could help stimulate changes in nutrition in much the same way the rise of gyms, exercise videos and sports, along with physical-education programs in schools, helped convince half of the adult population to exercise more.
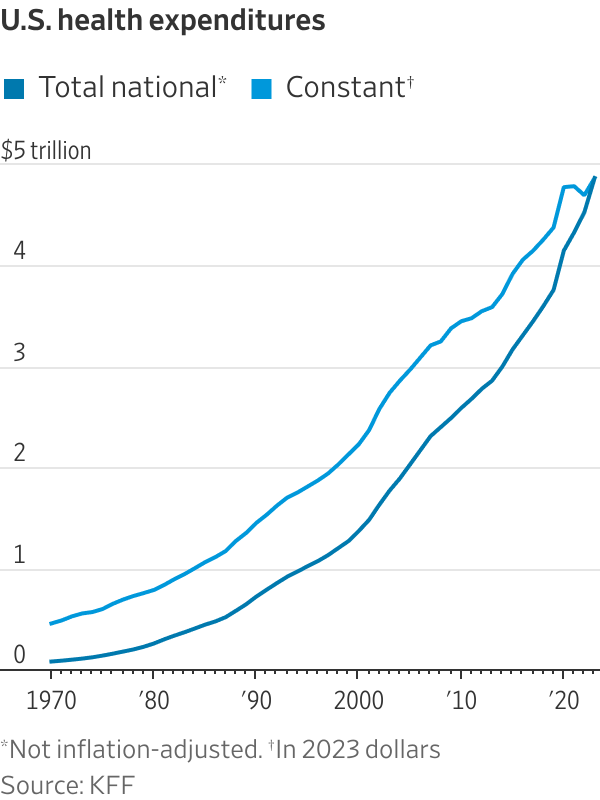
After decades of eating too much unhealthy food, the average middle-aged American is living with multiple chronic conditions and paying unsustainable healthcare costs to receive sick care. The U.S. could spend a lot less and achieve much better results with some of the changes we have outlined here, along with education starting at a young age.
Valter D. Longo is the Edna Jones professor in gerontology and director of the Longevity Institute, and Sebastian Brandhorst is a research assistant professor of gerontology, both at the University of Southern California’s Leonard Davis School of Gerontology.







